
East and South Africa Regional Cholera Platform
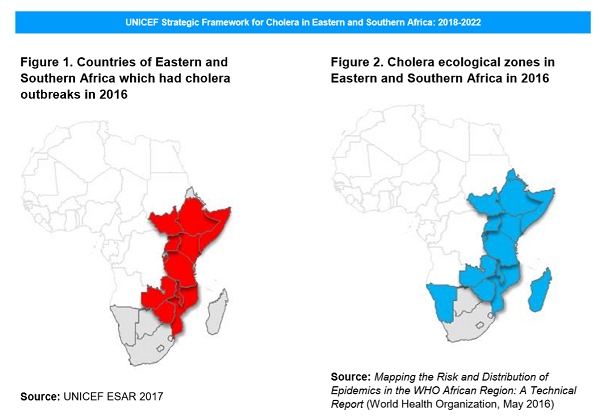
Cholera is endemic in at least half of the 21 countries in the UNICEF Eastern and Southern Africa region. In 2016, more than 70,000 cholera cases were reported in 12 countries in the region. The Eastern and Southern Africa region accounted for 68 per cent of cases reported in Africa as a whole, with just 4 East African countries making up 61 per cent of all cases reported in Africa: Ethiopia (31 per cent), Somalia (15 per cent), the United Republic of Tanzania (9 per cent) and Kenya (6 per cent). The case fatality rate in Eastern and Southern Africa was 1.5 per cent which is above the World Health Organisation (WHO) threshold of 1 per cent.
In highly endemic areas, a small number of specific geographic zones and populations are known as cholera ‘hotspots’. Such hotspots experience alternating seasonal outbreaks and lull periods and are thought to be the source of epidemics that spread beyond their boundaries. For example, frequent outbreaks among the fishing communities of Lake Malawi seem to be the origin of cholera transmission in Malawi. Cholera hotspots have also been identified in parts of the Great Lakes region, including several in the Democratic Republic of the Congo: on Lake Kivu bordering Rwanda; on Lake Tanganyika which borders Burundi, the United Republic of Tanzania, and Zambia; and on Lake Albert and border districts in Uganda. These hotspots have been associated with both in-country and cross-border spread of cholera within the region.
Drivers of cholera in the region include insufficient access to safe drinking water and adequate basic sanitation, as well as poor hygiene practices. Population displacements, whether due to conflict and instability or environmental and weather-related causes, are a major factor contributing to the persistence of the disease. With increased mobility of populations, cholera outbreaks can spread easily between countries, especially in high-risk epidemiological basins. The 2009–2010 Zimbabwe outbreak which spread across all countries of southern Africa bar Lesotho is an example, as are outbreaks in camps hosting South Sudanese refugees in Uganda (2016) and Burundian refugees in the United Republic of Tanzania (2015). Cholera control can be particularly challenging in the context of protracted emergencies, as in Somalia where in 2016 severe drought conditions exacerbated the incidence of malnutrition among the population; more than 1 million people were in urgent need of water, sanitation, and hygiene (WASH) interventions; and insecurity continued to hamper humanitarian access to communities.
Regional initiatives
National governments and development partners undertake cholera initiatives on an annual basis, yet implementing capacity and effective strategies for cholera preparedness, prevention, response and control remain limited and cholera is not sufficiently curbed. Crossborder transmission is poorly addressed and governments are sometimes reluctant to report cholera cases, which leads to overall underestimation of the extent of the disease which impedes a timely and targeted response. A step change in terms of coordination is needed in order to bring about a watertight response.
Among some of the key challenges are: the lack of adequate national plans for cholera prevention and response and insufficient geographic focus and investment in known cholera hotspots, limited access to remote communities, complex social and anthropological norms, inadequate or non-existent cross-border collaboration mechanisms, limited local capacity in some technical areas, already highly vulnerable populations (for example nutritional issues) and insufficient engagement of communities and societies in cholera prevention, preparedness and response actions.
A successful approach to cholera prevention, preparedness and response requires a joint, multi-sectoral and comprehensive strategy that transcends borders and sectors and that has clear delineation of roles and responsibilities among all stakeholders. The emphasis should be on coordinated national and inter-country action and effective partnerships to get the job done. Tackling cholera requires teamwork across sectors and professions, including health and water, sanitation and hygiene, community mobilization and behaviour change. Lessons can be drawn from the experience of the Regional Cholera Platform operating in West and Central Africa and specific country based learning.
To know more about the epidemiological situation in ESAR and the work achieved, visit their webpage: https://www.humanitarianresponse.info/en/operations/southern-eastern-africa/regional-wash-cholera-page